
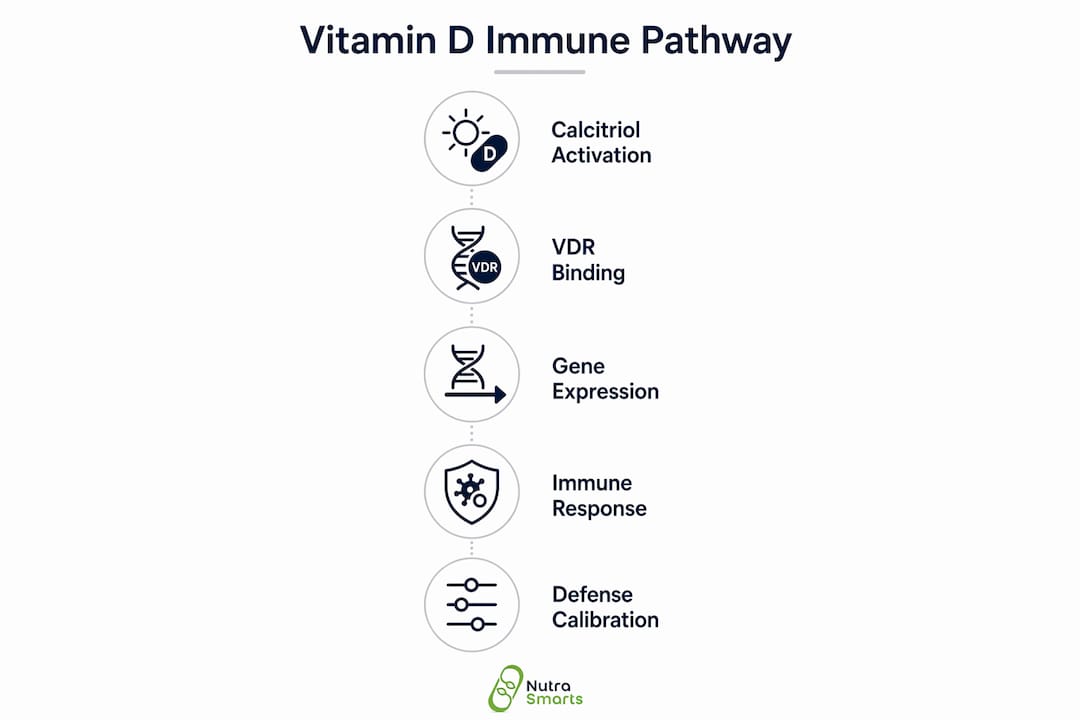
Vitamin D affects immune function primarily because its active metabolite, calcitriol, binds to vitamin D receptors (VDR) expressed on nearly every type of immune cell, directly altering gene expression and cytokine production. This makes vitamin D an immunomodulator, a term scientists use to describe compounds that regulate immune activity rather than simply stimulating or suppressing it. Unlike calcium absorption, which most people associate with vitamin D, its role in immunity operates more like a hormone than a traditional nutrient. Understanding why vitamin D affects immune function means tracing calcitriol's path from your bloodstream to the nucleus of a T cell, where it rewrites the instructions your immune system follows.
Why vitamin D affects immune function at the cellular level
The mechanism starts with VDR activation on immune cells, where calcitriol binds and triggers changes in gene expression that control how aggressively or cautiously the immune system responds. This is not a peripheral effect. Macrophages, dendritic cells, T cells, and B cells all carry VDR, meaning vitamin D has direct access to every major branch of your immune system.
What makes this especially significant is that immune cells do not rely solely on calcitriol produced by the kidneys. Research confirms that macrophages and dendritic cells express CYP27B1, the enzyme that converts inactive vitamin D into calcitriol locally at infection sites. This autocrine and paracrine signaling allows your immune system to activate vitamin D on demand, precisely where and when a pathogen is detected. The implication is that vitamin D's immune effects are context-dependent, not just a function of your blood level.
This dual activation system, systemic from the kidneys and local within immune tissue, explains why vitamin D deficiency creates such broad immune vulnerabilities. When circulating levels are low, both pathways are compromised simultaneously.

How does vitamin D enhance innate immune defenses?
The innate immune system is your body's first responder, and vitamin D directly strengthens several of its core tools.
- Antimicrobial peptide production: VDR activation triggers the production of cathelicidin and beta-defensins, proteins that punch holes in bacterial and viral membranes. This is one of the most direct ways vitamin D boosts antimicrobial defense without requiring prior exposure to a pathogen.
- Autophagy promotion: Vitamin D signals macrophages to engulf and destroy intracellular pathogens through autophagy, a cellular cleanup process that is particularly effective against Mycobacterium tuberculosis.
- Epithelial barrier integrity: Vitamin D maintains tight junction proteins in respiratory and gut epithelium, reducing the likelihood that pathogens breach the mucosal lining in the first place.
- Pathogen clearance speed: By priming macrophages before infection occurs, adequate vitamin D levels reduce the time between pathogen detection and neutralization.
The respiratory barrier effect deserves particular attention. Respiratory tissues are among the most VDR-dense in the body, which explains the consistent association between vitamin D deficiency and upper respiratory tract infections. When the epithelial barrier weakens due to low vitamin D, viruses gain easier entry into the bloodstream.
Pro Tip: If you are prone to seasonal respiratory infections, ask your doctor to test your 25-hydroxyvitamin D level before winter. Correcting a deficiency before cold and flu season is more effective than supplementing reactively.
How does vitamin D regulate adaptive immunity and prevent overactivation?
The adaptive immune system delivers targeted, long-term responses, but it can also overshoot and attack healthy tissue. Vitamin D's role here is to act as a brake on excessive inflammation while still allowing effective pathogen clearance.
- T-cell polarization: Vitamin D shifts T-cell responses away from pro-inflammatory Th1 and Th17 phenotypes toward regulatory T cells (Tregs). Th17 cells drive autoimmune inflammation in conditions like rheumatoid arthritis and multiple sclerosis. Tregs suppress this activity.
- Cytokine modulation: Calcitriol decreases production of IL-6, IL-17, and TNF-α, the cytokines most associated with tissue-damaging inflammation. Simultaneously, it increases IL-10, an anti-inflammatory cytokine that signals the immune system to stand down after a threat is cleared.
- Thymic tolerance: Vitamin D supports AIRE expression in thymic epithelial cells, a protein that teaches developing T cells to recognize and tolerate the body's own tissues. This is a central mechanism for preventing autoimmunity.
- Dendritic cell maturation: Vitamin D shifts dendritic cells toward a tolerogenic state, meaning they present antigens in a way that promotes tolerance rather than aggressive immune activation.
This balance is what makes vitamin D genuinely unique among immune-relevant nutrients. Zinc and vitamin C primarily support immune activation. Vitamin D does that too, but it simultaneously prevents the immune system from destroying the host in the process.
Pro Tip: Readers managing autoimmune conditions should explore the Vitamin D vs Vitamin K2 comparison at Nutrasmarts, since K2 influences where calcium is deposited and may interact with vitamin D's broader physiological effects.
What are the clinical impacts of vitamin D deficiency on immune health?
The clinical evidence connecting vitamin D deficiency and immune dysfunction is substantial, though not without nuance.
| Condition | Observed association with low vitamin D |
|---|---|
| Multiple sclerosis | Higher incidence in populations with limited sun exposure and low serum 25(OH)D |
| Lupus (SLE) | Deficiency correlates with increased disease activity and flares |
| Respiratory infections | Low levels associated with higher rates of influenza and COVID-19 severity |
| Inflammatory bowel disease | Impaired Treg function linked to reduced mucosal tolerance |
Vitamin D deficiency favors pro-inflammatory immune shifts because impaired Treg function allows Th1 and Th17 responses to dominate unchecked. This creates a chronic low-grade inflammatory state that raises the risk of both infection and autoimmune disease simultaneously.
The COVID-19 pandemic generated a large body of observational data on this relationship. Patients with severe COVID-19 outcomes consistently showed lower 25-hydroxyvitamin D levels than those with mild illness. This does not prove causation, but it aligns precisely with the known mechanism: vitamin D deficiency weakens epithelial barriers, reduces cathelicidin production, and removes the Treg brake on cytokine storms.
For autoimmune conditions specifically, the connection between deficiency and autoimmunity is increasingly recognized across dermatological and systemic conditions alike. The common thread is impaired immune tolerance when vitamin D signaling is absent.
Why do vitamin D supplementation studies show mixed results?
If the mechanism is so clear, why do clinical trials produce inconsistent outcomes? Several factors explain the gap between biological plausibility and trial results.
- Baseline status determines benefit: Supplementation benefits are threshold-dependent. Individuals who are already sufficient in vitamin D see minimal immune improvement from additional supplementation. Most of the measurable benefit accrues to those correcting a true deficiency.
- Dose and regimen matter: A meta-analysis of 17 RCTs found that low-dose daily vitamin D at or below 1,000 IU per day reduced acute respiratory infections, while high-dose bolus regimens showed no benefit. This suggests that mimicking natural daily sun exposure is more effective than periodic megadoses.
- Population heterogeneity: Trials mixing replete and deficient participants dilute the signal. A trial where 60% of participants already have adequate levels will show weak average effects even if deficient participants benefit substantially.
- Biomarker versus clinical outcome gap: Immune biomarker changes induced by vitamin D, such as shifts in cytokine profiles or Treg counts, do not always translate into measurable reductions in disease incidence. Immune diseases are complex, and a single nutrient rarely moves the needle on a clinical endpoint alone.
The practical takeaway is that vitamin D supplementation is not a universal immune booster. It is a correction tool. Its power lies in restoring function that deficiency has impaired, not in supercharging an already sufficient immune system.
How can individuals optimize vitamin D for immune health?
Optimizing vitamin D for immune health requires knowing your baseline, not guessing at it.
The standard recommendation from most health authorities is a serum 25-hydroxyvitamin D level between 30 and 50 ng/mL for general health. Immune benefits appear most consistently above 30 ng/mL, and levels below 20 ng/mL are classified as deficient. For supplementation, most adults require between 1,500 and 2,000 IU daily to maintain sufficiency, though individuals with obesity, darker skin tones, or limited sun exposure often need more.
Sunlight remains the most efficient source. Twenty minutes of midday sun exposure on arms and legs produces roughly 10,000 to 20,000 IU in fair-skinned individuals, though this drops sharply in winter months above 35 degrees latitude. Supplementation becomes necessary for most people in northern climates from October through March.
Fat-soluble vitamin D3 (cholecalciferol) raises serum levels more effectively than D2 (ergocalciferol), making it the preferred supplementation form. Taking it with a meal containing fat improves absorption by roughly 30 to 50 percent. For a detailed breakdown of vitamin D dosage and research, Nutrasmarts maintains a peer-reviewed ingredient profile with clinical trial citations.
Pro Tip: Routine testing is worth the cost for at-risk groups, including adults over 60, people with inflammatory bowel disease, and those who work indoors year-round. A single blood test costs less than three months of unnecessary supplementation.
Key takeaways
Vitamin D affects immune function by acting as a hormone-like regulator that strengthens antimicrobial defenses, shifts T-cell responses toward tolerance, and prevents the inflammatory overactivation that drives autoimmune disease.
| Point | Details |
|---|---|
| Calcitriol drives the mechanism | Vitamin D's active form binds VDR on immune cells to control gene expression and cytokine output. |
| Innate and adaptive immunity both respond | Vitamin D induces cathelicidin, supports Tregs, and reduces pro-inflammatory cytokines like IL-6 and TNF-α. |
| Deficiency creates dual risk | Low vitamin D raises both infection susceptibility and autoimmune disease risk through impaired Treg function. |
| Supplementation is threshold-dependent | Benefits are strongest in deficient individuals; replete individuals see limited immune improvement from extra doses. |
| Low daily doses outperform megadoses | Daily supplementation at or below 1,000 IU reduces respiratory infections more reliably than high-dose bolus regimens. |
The nuance most people miss about vitamin D and immunity
At Nutrasmarts, we review hundreds of supplement ingredient profiles each year, and vitamin D generates more misunderstanding than almost any other compound. The most common mistake is treating it as an immune stimulant, something you take to give your immune system a boost the way caffeine boosts energy. That framing is wrong, and it leads people to either over-supplement when they are already sufficient or to expect protection that vitamin D cannot provide alone.
What vitamin D actually does is closer to calibration. It raises your immune system's capacity to detect and destroy pathogens while simultaneously preventing the inflammatory cascade from spiraling into tissue damage. That dual function is rare. Most immune-relevant nutrients do one or the other.
The research we find most compelling in 2026 is the local activation data. The fact that macrophages produce their own calcitriol at infection sites means vitamin D's immune effects are not purely dependent on your serum level. This is why two people with identical blood levels can have different immune outcomes. Context, genetics, and the specific immune challenge all interact with vitamin D signaling in ways that a single blood test cannot capture.
Our honest recommendation: test before you supplement, correct a deficiency if you have one, and do not expect vitamin D to replace sleep, exercise, or a diet with adequate zinc and vitamin C. It is one critical input in a system that requires many.
— NutraSmarts
Find the right immune support supplement for your needs
Knowing the science behind vitamin D and immune function is the first step. Finding a supplement that matches your specific deficiency profile and health goals is the next one. Nutrasmarts has reviewed over 130 immune support products against peer-reviewed clinical evidence, so you are not choosing based on marketing claims. Every product in the best immune support supplements category is evaluated for ingredient quality, dosage accuracy, and clinical backing. If you are also managing metabolic health alongside immunity, the metabolic health supplements category includes vitamin D products with verified third-party testing and FDA-compliant labeling data.
FAQ
What does vitamin D actually do to the immune system?
Vitamin D's active form, calcitriol, binds to VDR on immune cells and alters gene expression to regulate both innate and adaptive immune responses. This includes triggering antimicrobial peptide production, shifting T cells toward regulatory phenotypes, and reducing pro-inflammatory cytokines like IL-6 and TNF-α.
Can low vitamin D cause more frequent infections?
Yes. Vitamin D deficiency impairs cathelicidin production and weakens epithelial barriers, both of which are frontline defenses against respiratory pathogens. Observational data from influenza and COVID-19 studies consistently links lower 25-hydroxyvitamin D levels to higher infection rates and more severe outcomes.
How much vitamin D should I take for immune health?
Most adults need 1,500 to 2,000 IU of vitamin D3 daily to maintain serum levels above 30 ng/mL, the threshold where immune benefits are most consistently observed. Testing your baseline level first is the most reliable way to determine the right dose for your situation.
Why do some vitamin D studies show no immune benefit?
Supplementation trials show mixed results primarily because benefits are threshold-dependent. Individuals who are already sufficient in vitamin D see little additional immune improvement, and many trials mix deficient and replete participants, which dilutes the measurable effect across the study group.
Is vitamin D3 better than D2 for immune support?
Vitamin D3 (cholecalciferol) raises serum 25-hydroxyvitamin D levels more effectively than D2 (ergocalciferol) and is the preferred form for supplementation. Taking D3 with a fat-containing meal improves absorption and is the standard recommendation from most clinical guidelines.