Supplement absorption is defined as the process by which nutrients pass from the digestive tract into the bloodstream, where they become available for the body to use. This process, formally called bioavailability in pharmacology and nutrition science, determines whether a supplement actually works or simply gets excreted. Supplement absorption mechanisms explained across five distinct physiological pathways show why two products with identical milligram doses can produce completely different results. The chemical form of a nutrient, the food you eat with it, and your individual physiology all shape how much of a dose reaches your tissues. Understanding these mechanisms is the clearest path to spending less and getting more from every supplement you take.
What are the main supplement absorption mechanisms in the body?
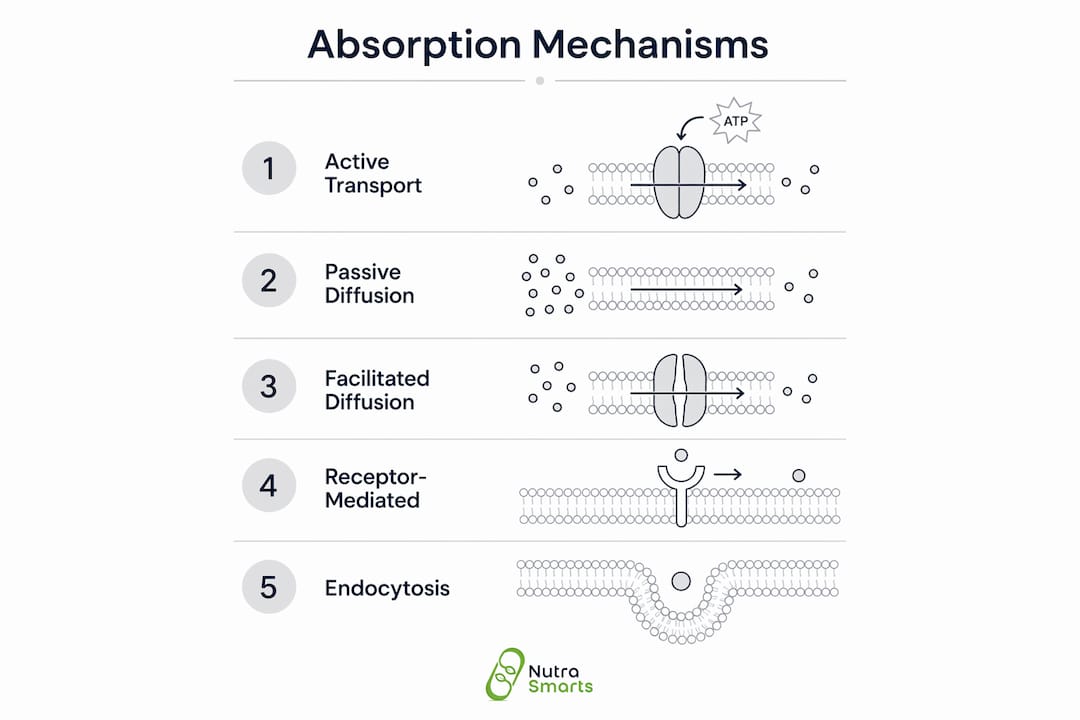
The body uses five primary pathways to move nutrients from the gut into circulation: active transport, passive diffusion, facilitated diffusion, endocytosis, and receptor-mediated transport. Each pathway suits different nutrient types, and knowing which one applies tells you a great deal about how to take a supplement correctly.
Active transport moves nutrients against a concentration gradient using energy and specific carrier proteins. Vitamin C travels via SVCT (sodium-dependent vitamin C transporter) proteins, which saturate at high doses. That saturation explains why only about 30% of a large vitamin C dose is bioavailable. The rest exits through urine.

Passive diffusion requires no energy. Fat-soluble compounds dissolve into the lipid membrane of intestinal cells and pass through freely, which is why vitamins A, D, E, and K absorb well when dietary fat is present. Facilitated diffusion uses carrier proteins but no energy, and it moves nutrients down a concentration gradient. Many B vitamins use this route at moderate doses.
Receptor-mediated transport is the most selective pathway. Vitamin B12 is the clearest example: it binds to intrinsic factor in the stomach, and the resulting complex attaches to CUBAM receptors in the ileum for absorption. Without intrinsic factor, oral B12 absorption drops to a fraction of a percent. Endocytosis handles larger molecules by engulfing them into vesicles, and it plays a role in absorbing some immunoglobulins and intact proteins.
The small intestine is where nearly all of this happens. Its absorptive surface spans roughly 30 square meters, thanks to villi and microvilli. That surface area is a biological asset, but it only works if the nutrient arrives in a form the relevant transporter recognizes.
Pro Tip: Absorption and bioavailability are not the same thing. A nutrient can cross the gut wall and still lose potency to hepatic first-pass metabolism before reaching target tissues. Always check whether a supplement's efficacy data measures gut absorption or systemic availability.
How does chemical form affect how supplements are absorbed?
Bioavailability depends more on chemical form than on milligram dose. This single fact separates effective supplementation from expensive guesswork.
Water-soluble vs. fat-soluble vitamins
Water-soluble vitamins, including vitamin C and the B-complex group, dissolve in water and enter the bloodstream directly through intestinal cells. The body does not store them in significant amounts, so excess is excreted quickly. Fat-soluble vitamins, including A, D, E, and K, require bile acids and dietary fats to form micelles, tiny lipid droplets that carry the vitamins into lymphatic vessels before reaching circulation. Fat-soluble vitamin absorption drops sharply without dietary fat present, which is why taking vitamin D on an empty stomach is a common and costly mistake.
Mineral form and chelation
The form of a mineral changes which transporter it uses and how well it survives the digestive environment. Magnesium oxide, one of the cheapest and most common forms, has low solubility in the gut and poor absorption. Magnesium glycinate, a chelated form where magnesium is bound to the amino acid glycine, uses amino acid transporters in the intestinal wall. Those transporters are more abundant and less competitive than the mineral-specific channels magnesium oxide depends on.
Chelation works because it wraps a mineral in an organic molecule, protecting it from binding to inhibitors like phytates and oxalates in food. Bisglycinate chelates use amino acid transporters to improve mineral uptake, bypassing the bottleneck of shared mineral channels. The same logic applies to iron bisglycinate versus ferrous sulfate, and zinc bisglycinate versus zinc oxide.
Folate offers another clear example. Folic acid, the synthetic form, requires enzymatic conversion to methylfolate before the body can use it. People with MTHFR gene variants convert folic acid slowly, which means a standard folic acid supplement may deliver far less active folate than the label suggests. Methylfolate skips that conversion step entirely, making it more bioavailable for anyone, and especially for those with MTHFR polymorphisms.
Pro Tip: When comparing two mineral supplements, ignore the milligram count and look at the form first. A 100 mg dose of magnesium glycinate delivers more usable magnesium than a 400 mg dose of magnesium oxide for most people.
What factors influence real-world supplement absorption and bioavailability?
Understanding nutrient absorption in a lab setting is one thing. Real-world uptake depends on a web of interacting variables that most supplement labels never mention.
Food context and nutrient interactions
What you eat alongside a supplement changes its absorption dramatically. Vitamin C improves non-heme iron absorption by chemically reducing ferric iron (Fe3+) to ferrous iron (Fe2+), the form intestinal transporters prefer. Calcium does the opposite: it competes with iron at shared transport sites and reduces iron uptake. Taking an iron supplement with a glass of milk is a reliable way to blunt its effect.
Phytates, found in whole grains, legumes, and seeds, bind to zinc, iron, calcium, and magnesium in the gut and block their absorption. This is not a reason to avoid whole foods, but it is a reason to time mineral supplements away from high-phytate meals when absorption matters most.
Competitive inhibition among minerals
Calcium, iron, zinc, and magnesium share transport pathways, and they compete when taken together. Taking a calcium supplement at the same time as an iron supplement reduces the absorbed amount of both. Spacing mineral supplements by two to three hours removes most of that competition and improves uptake for each.
First-pass metabolism
Even after a nutrient crosses the gut wall, the liver can intercept and metabolize it before it reaches systemic circulation. Hepatic first-pass metabolism reduces the effective dose of many compounds, including some herbal extracts and fat-soluble nutrients. This is why gut absorption data alone does not predict how much of a supplement reaches muscle, bone, or brain tissue.
Individual variability
Age reduces stomach acid production, which impairs B12 absorption and lowers mineral solubility. Gut inflammation or conditions like Crohn's disease damage the intestinal villi that handle absorption. Genetics, particularly MTHFR polymorphisms, alter how efficiently the body converts certain vitamin forms. Delivery format also matters: liquid supplements may absorb more quickly than tablets, though not all nutrients can be formulated as liquids, and probiotics often require protective capsule coatings to survive stomach acid.
Pro Tip: If you take multiple mineral supplements daily, split them across two separate meals. This one habit can meaningfully improve what you actually absorb from each.
How do absorption mechanisms translate into practical supplement use?
Knowing the science behind how supplements are absorbed is only useful if it changes what you do. These principles translate directly into better purchasing and dosing decisions.
-
Take fat-soluble vitamins with a fat-containing meal. Vitamins A, D, E, and K need bile acids and dietary fat to form the micelles that carry them into lymphatic vessels. A meal with avocado, olive oil, or eggs provides enough fat to support this process. Taking these vitamins on an empty stomach wastes a significant portion of the dose.
-
Choose form over milligrams. A supplement with a lower dose in a highly bioavailable form outperforms a high-dose product in a poorly absorbed form. Magnesium glycinate, methylfolate, and iron bisglycinate are examples where form selection matters more than the number on the label. Nutrasmarts maintains a database of over 800 ingredients with peer-reviewed citations to help you compare forms by evidence, not marketing.
-
Space mineral supplements to reduce competition. Iron, zinc, calcium, and magnesium compete for the same transporters. Taking them at separate meals reduces that competition and improves absorption for each mineral individually.
-
Pair iron supplements with vitamin C. Vitamin C converts non-heme iron to its absorbable form. A simple glass of orange juice or a vitamin C tablet taken alongside an iron supplement measurably improves uptake.
-
Account for your personal biology. Older adults, people with gut conditions, and those with known genetic variants like MTHFR need to select supplement forms that bypass the conversion steps their bodies handle poorly. The label dosage is not equal to the absorbed amount for anyone, and that gap widens with age and gut dysfunction.
Understanding why supplement dosage matters goes beyond reading the milligram count. The absorbed fraction is what drives outcomes, and that fraction is shaped by form, food, timing, and individual physiology working together.
Key Takeaways
Bioavailability, not milligram dose, is the true measure of supplement effectiveness, and it is determined by absorption pathway, chemical form, food context, and individual physiology.
| Point | Details |
|---|---|
| Absorption pathway determines uptake | Each nutrient uses a specific route: active transport, passive diffusion, or receptor-mediated transport. |
| Chemical form drives bioavailability | Chelated minerals and active vitamin forms absorb better than cheap oxide or synthetic alternatives. |
| Food context changes absorption | Fat-soluble vitamins need dietary fat; vitamin C boosts iron uptake; calcium blocks it. |
| Minerals compete for transporters | Space calcium, iron, zinc, and magnesium across separate meals to improve each one's uptake. |
| First-pass metabolism reduces effective dose | Gut absorption does not equal systemic availability; the liver metabolizes many nutrients before they reach tissues. |
The dose on the label is the least important number
At Nutrasmarts, we review hundreds of supplement formulations every year, and the pattern we see most often is this: people buy the highest milligram dose they can find and assume that means the strongest effect. It does not. The milligram count tells you what went into the capsule. It says nothing about what reaches your bloodstream.
The gap between label dose and absorbed amount is where most supplement money is wasted. A 500 mg magnesium oxide tablet may deliver less usable magnesium than a 150 mg magnesium glycinate capsule. A standard folic acid supplement may do almost nothing for someone with an MTHFR variant, while methylfolate at a lower dose works immediately. These are not edge cases. They are the norm.
What we find most underappreciated is the role of the food matrix. "Take with food" is not specific enough advice. The type of food changes the outcome. Fat-soluble vitamins need fat. Iron needs vitamin C and needs to be separated from calcium. Minerals need distance from phytate-rich foods. The food matrix surrounding a supplement dose can dramatically shift absorption in either direction.
The science of supplement absorption is still evolving. Personalized supplementation, guided by genetics, gut health markers, and blood levels, is where the field is heading. Until that becomes standard practice, the best approach is to choose evidence-backed forms, time your doses thoughtfully, and treat the label as a starting point rather than a guarantee.
— Nutrasmarts
How Nutrasmarts supports smarter supplement decisions
Choosing the right supplement form is harder than it should be. Most labels highlight milligrams, not mechanisms.
Nutrasmarts cuts through that noise with a science-backed ingredient database covering over 800 ingredients, each linked to peer-reviewed studies and clinical trial citations. You can search by health concern, compare ingredient forms by absorption evidence, and find formulations that match your goals. For those focused on metabolic health, the top-reviewed metabolic supplements page applies these exact absorption criteria to 130 reviewed products. Every recommendation accounts for bioavailability, not just dose. That is the difference between a supplement that works and one that does not.
FAQ
What is bioavailability in supplements?
Bioavailability is the fraction of an ingested nutrient that reaches systemic circulation in an active form. It is the true measure of supplement effectiveness, not the milligram dose listed on the label.
Why does supplement form matter more than dose?
Chemical form determines which absorption pathway a nutrient uses. Chelated minerals like magnesium glycinate use amino acid transporters with higher capacity, while oxide forms rely on less efficient mineral channels, resulting in lower uptake at the same dose.
Should I take supplements with food?
Fat-soluble vitamins (A, D, E, K) require a fat-containing meal for proper absorption via micelle formation. Water-soluble vitamins absorb well with or without food, though taking them with a meal often reduces stomach discomfort.
Can taking multiple supplements together reduce their effectiveness?
Yes. Calcium, iron, zinc, and magnesium compete for shared transporters, so taking them simultaneously reduces absorption for each. Spacing mineral supplements by two to three hours across separate meals improves uptake.
What is first-pass metabolism and why does it matter?
First-pass metabolism is the liver's rapid processing of absorbed compounds before they reach systemic circulation. A nutrient that crosses the gut wall efficiently can still have low systemic availability if the liver breaks it down quickly, which is why gut absorption data alone does not predict real-world supplement effects.