Cohort studies are defined as observational research designs that follow a group of people over time to measure how exposures relate to health outcomes. The role of cohort study supplement evidence is to provide longitudinal, real-world data that no short-term trial can replicate. Prospective cohort studies rank below RCTs but above case-control and cross-sectional designs in the evidence hierarchy, making them a foundational tool in supplement efficacy research. For researchers and graduate students in nutritional epidemiology, understanding how cohort data contributes to and where it falls short of causal proof is not optional. It is the difference between drawing sound conclusions and overclaiming from observational signals.
How do cohort studies contribute uniquely to supplement evidence?
Cohort studies generate supplement evidence in ways that randomized controlled trials simply cannot. Their defining strength is temporality: participants are free of the outcome at baseline and followed forward in time, which means researchers can confirm that supplement exposure preceded any observed health change. That sequencing is a prerequisite for causal reasoning under the Bradford Hill criteria.
Three specific contributions set cohort designs apart from other observational methods:
- Incidence and relative risk calculation. Cohort studies directly measure how often an outcome occurs in exposed versus unexposed groups. This produces relative risk estimates that case-control studies can only approximate with odds ratios.
- Long-term and ethically constrained exposures. Randomizing people to years of supplement use or deprivation is often impractical or unethical. Cohort studies observe these exposures as they occur naturally in populations.
- Dose-response tracking. Researchers can record supplement dosage over time and test whether higher doses correlate with stronger effects, a pattern that strengthens biological plausibility arguments.
- Real-world population diversity. Large cohorts capture demographic variation that tightly controlled trials exclude, improving external validity for public health recommendations.
The omega-3 literature illustrates these strengths clearly. Long-term follow-up provides unique insights on supplement effects on chronic disease progression in ways that short trials cannot capture. A multi-year cohort tracking daily omega-3 intake alongside cognitive assessments can detect gradual neurological changes that a 12-week RCT would miss entirely.
Pro Tip: When evaluating a cohort study on supplements, check whether the exposure was measured repeatedly throughout follow-up or only at baseline. Single-point exposure measurement misclassifies participants who change their supplement habits, which biases results toward the null.

Cohort studies also serve as hypothesis generators. When a large, well-conducted cohort finds a consistent association between a supplement and a health outcome, that signal justifies the investment in a full RCT. Without cohort evidence, clinical trial funding bodies would have far less direction on which supplements merit rigorous testing.
What are the limitations and biases in cohort supplement studies?
Cohort studies cannot establish causation alone. The lack of randomization means that supplement users and non-users differ in ways beyond the supplement itself, and those differences can explain observed associations entirely.
The most consequential bias in supplement cohort research is healthy-user bias. People who take supplements regularly tend to exercise more, eat better, smoke less, and visit doctors more often. After adjusting for these lifestyle factors, CVD incidence rate ratios in supplement cohorts approach null (1.008; 95% CI 0.900, 1.128). That finding means the apparent protective effect of many supplements in unadjusted analyses is largely a reflection of who takes them, not what the supplements do.
Additional sources of bias that researchers must account for include:
- Confounding by socioeconomic status. Higher-income groups use supplements more and also have better health outcomes for unrelated reasons.
- Loss to follow-up and attrition bias. Participants who drop out of long cohorts are rarely a random subset. Sicker or less health-conscious individuals leave disproportionately, distorting results.
- Generalizability gaps. A cohort drawn from nurses, physicians, or a single geographic region may not represent the broader population for whom supplement recommendations are made.
- Recall and measurement error. Self-reported supplement use is prone to inaccuracy, particularly for dosage and consistency.
One underused tool for quantifying confounding is the negative-control outcome framework. Applying Lipsitch's negative-control framework to datasets like NHANES III allows researchers to estimate the minimum confounding floor in a supplement-outcome association. If a supplement shows a strong association with an outcome it biologically cannot affect, that association is a confounding signal, not a real effect.
Pro Tip: Before accepting a cohort finding on a supplement, look for whether the authors tested a negative-control outcome. Its absence does not invalidate the study, but its presence significantly strengthens the credibility of the reported associations.
Single cohort findings always need corroboration. Experts recommend treating cohort studies as supportive evidence requiring convergence across multiple studies and clinical trials before drawing efficacy conclusions.
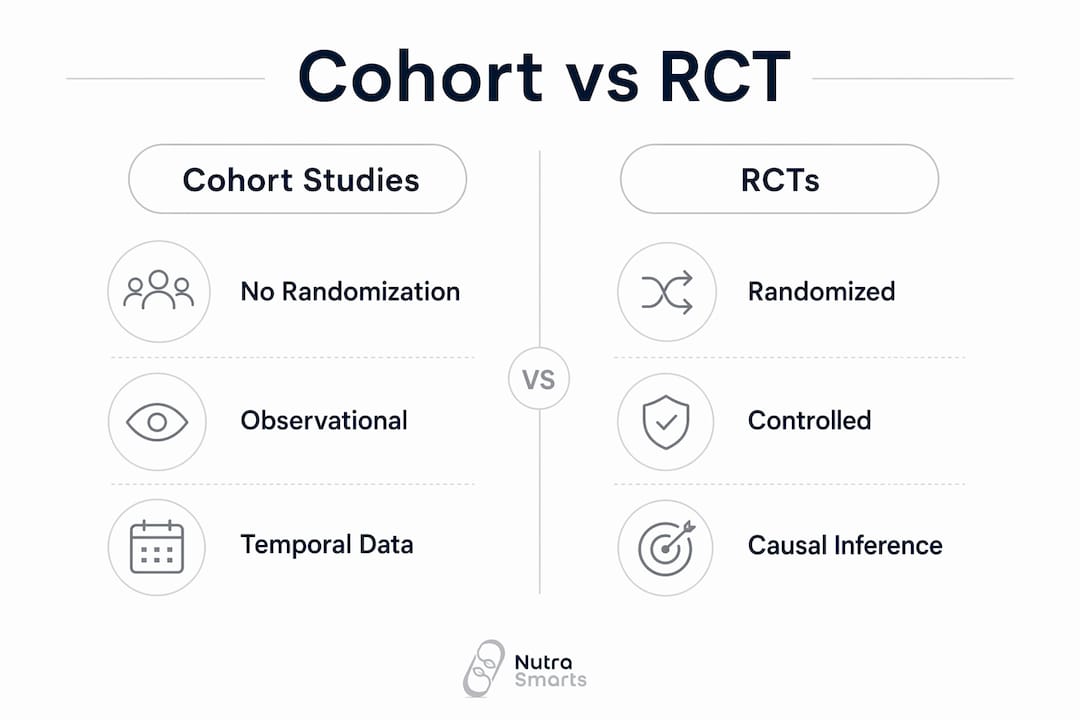
How does cohort evidence compare to RCT findings in supplement research?
The relationship between cohort studies and RCTs is more nuanced than a simple hierarchy suggests. A meta-epidemiological analysis of 64 closely matched RCT-cohort pairs found that roughly 83% of pairs showed directional agreement on nutritional supplement outcomes. That figure sounds reassuring until you examine what it conceals.
| Feature | Cohort studies | Randomized controlled trials |
|---|---|---|
| Randomization | No | Yes |
| Causal inference strength | Moderate | High |
| Follow-up duration | Often years to decades | Typically weeks to months |
| Real-world applicability | High | Lower (controlled conditions) |
| Ethical feasibility for long exposures | High | Often limited |
| Bias control | Depends on design quality | Stronger by design |
The 83% directional agreement does not mean individual pairs are interchangeable. Pooled summary measures near 1.0 mask large within-pair variability, and discrepancies between individual cohort and RCT findings remain around 31%. A researcher who assumes a cohort finding will replicate in a trial is taking a meaningful risk.
Heterogeneity between cohort and RCT results often traces back to follow-up duration and population differences. A cohort tracking vitamin D intake over 10 years in community-dwelling older adults will produce different effect estimates than a 6-month RCT in a clinical population. Neither is wrong. They are answering different questions about the same supplement.
The Bradford Hill criteria provide the interpretive framework for bridging this gap. Strength of association, consistency across studies, biological plausibility, and dose-response relationships all contribute to causal inference when randomization is absent. Applying these criteria to cohort data alongside supplement efficacy measurement tools gives researchers a structured way to weigh observational evidence without overclaiming.
Pro Tip: When a cohort finding and an RCT disagree on a supplement outcome, do not automatically defer to the RCT. Check whether the populations, dosages, and follow-up periods are actually comparable. Discordance often reflects design differences, not contradictory biology.
What practical steps help researchers evaluate cohort supplement evidence?
Critical appraisal of cohort studies follows a consistent checklist regardless of the supplement being studied.
- Assess study design quality. Prospective cohorts are stronger than retrospective ones because exposure data is collected before outcomes occur. Check whether the study used validated dietary assessment tools or relied on single-point self-report.
- Examine sample size and follow-up length. Small cohorts with short follow-up periods produce unstable risk estimates. For chronic disease outcomes, follow-up under five years rarely captures meaningful supplement effects.
- Identify confounders and their adjustment. A well-conducted cohort reports which confounders were measured and how they were handled statistically. Unadjusted analyses in supplement research are almost always misleading.
- Check for bias quantification. Look for sensitivity analyses, negative-control outcomes, or E-value calculations that estimate how strong an unmeasured confounder would need to be to explain the observed association.
- Triangulate with other evidence types. Cohort findings gain credibility when they align with mechanistic studies, double-blind supplement trials, and systematic reviews. No single cohort study should drive a clinical recommendation alone.
Applying cohort findings in clinical or public health settings requires the same caution. A cohort association between a supplement and reduced disease risk is a signal worth investigating, not a prescription. Communicating that distinction clearly is part of responsible evidence translation.
Pro Tip: Use the E-value when a cohort study lacks a negative-control outcome. The E-value tells you the minimum strength an unmeasured confounder would need to explain away the observed association. A high E-value means the finding is harder to dismiss as confounding.
Case study: omega-3 cohort evidence and cognitive function
The omega-3 and cognitive function literature is one of the clearest demonstrations of what cohort studies contribute to supplement evidence. An 8-year cohort study with 4,949 participants aged 60 and older found that daily omega-3 supplement use was associated with significant memory improvement (β = 1.050, 95% CI 0.643–1.456, p < .001). That effect size held after adjustment for age, sex, education, and baseline cognitive status.
The study's strengths are worth naming specifically. A sample of nearly 5,000 older adults followed for eight years provides statistical power and follow-up length that short trials cannot match. The longitudinal design captured gradual cognitive trajectories rather than snapshot differences, which is exactly the kind of data that cohort studies do better than any other design.
"Cohort studies serve as the primary observational bridge in supplement research by establishing exposure before outcome presence, vital for temporality assessments." — Epidemiological significance of cohort studies
The caveats are equally instructive. Self-reported supplement use introduces measurement error. Participants who consistently take omega-3s may differ from non-users in diet quality, physical activity, and social engagement, all of which independently protect cognitive function. The association is compelling, but it requires corroboration from clinical trials on supplement safety and mechanistic research on DHA's role in neuronal membrane integrity before causation can be claimed.
Researchers who want to examine the full omega-3 evidence base, including peer-reviewed citations on dosage and biological mechanisms, can review the omega-3 ingredient profile on Nutrasmarts. The database links directly to the studies underlying each claim, which makes evidence triangulation faster and more systematic.
Key takeaways
Cohort studies are indispensable for supplement research but require integration with RCTs, mechanistic data, and bias quantification tools to support causal conclusions.
| Point | Details |
|---|---|
| Temporality is the core strength | Cohort studies confirm supplement exposure precedes outcomes, satisfying a key Bradford Hill criterion. |
| Healthy-user bias is the primary threat | After lifestyle adjustment, many supplement associations approach null, signaling confounding rather than real effects. |
| 83% RCT-cohort directional agreement | Most cohort-RCT pairs agree on direction, but individual pair discordance around 31% limits direct interchangeability. |
| Negative-control outcomes quantify confounding | Applying this framework to supplement cohorts reveals the minimum confounding floor before accepting an association. |
| Triangulation is non-negotiable | No single cohort finding should drive supplement recommendations without convergent evidence from trials and mechanistic research. |
The uncomfortable truth about cohort evidence in supplement research
At Nutrasmarts, we review supplement research daily, and the pattern is consistent: cohort studies are both the most cited and the most misread evidence type in the supplement space. Researchers and students often treat a large, long-running cohort finding as near-equivalent to a positive RCT. It is not.
What cohort studies do exceptionally well is generate signals over time. The omega-3 and cognitive function data is a perfect example. Eight years, nearly 5,000 participants, a statistically significant memory association. That is a signal worth taking seriously. It is not proof of causation, and presenting it as such does real harm to scientific credibility.
The healthy-user bias problem is more severe in supplement research than in pharmaceutical research. People who choose to take supplements are systematically different from those who do not, and those differences are hard to fully measure or adjust for. A confounding floor analysis is not a perfect solution, but it is far better than assuming adjustment variables capture everything relevant.
My honest recommendation: treat every cohort finding on a supplement as a hypothesis with supporting evidence, not a conclusion. The Bradford Hill criteria exist precisely for this situation. Apply them. Ask whether the association is strong, consistent across populations, biologically plausible, and dose-dependent. If the answer to most of those questions is yes, the cohort finding deserves serious weight. If not, it deserves skepticism regardless of sample size.
Students especially need to resist the pull of impressive numbers. A cohort of 50,000 with a p-value of 0.001 can still be entirely explained by confounding. Statistical significance is not the same as scientific significance, and it is certainly not the same as clinical relevance.
— Nutrasmarts
Nutrasmarts: research tools built for supplement evidence
Evaluating supplement evidence means working across cohort studies, RCTs, and mechanistic research simultaneously. Nutrasmarts is built for exactly that workflow.
The Nutrasmarts database covers over 800 ingredients, each linked to peer-reviewed studies and clinical trial citations. Researchers can search supplements by symptom to find ingredients with the strongest evidence base for specific health concerns, from cognitive function to joint health. Every ingredient page organizes cohort findings, RCT data, and mechanistic evidence in one place, so triangulation does not require hours of database searching. The Supplement Facts Tool adds FDA-compliant label generation for researchers moving from evidence review into product development. For anyone serious about supplement evidence, Nutrasmarts cuts the time between finding a study and understanding what it actually means.
FAQ
What is the role of cohort studies in supplement evidence?
Cohort studies establish temporal associations between supplement use and health outcomes by following participants prospectively over time. They generate relative risk estimates and dose-response data that inform both clinical guidelines and RCT design.
How does healthy-user bias affect supplement cohort findings?
Healthy-user bias causes supplement users to appear healthier than non-users due to correlated lifestyle factors. After full adjustment, many supplement-outcome associations in cohort data shrink substantially or disappear entirely.
Do cohort studies and RCTs agree on supplement outcomes?
Approximately 83% of closely matched cohort-RCT pairs show directional agreement on nutritional outcomes, but individual pair discordance remains around 31%. Agreement on direction does not mean agreement on effect size.
Can a single cohort study prove a supplement works?
No. Cohort studies cannot establish causation due to the absence of randomization. A single cohort finding requires corroboration from multiple studies, RCTs, and mechanistic research before supporting an efficacy claim.
What is the Bradford Hill criteria and why does it matter for cohort studies?
The Bradford Hill criteria are a set of principles including strength, consistency, and biological plausibility used to evaluate whether an observed association is likely causal. They are the primary interpretive framework for drawing causal inferences from cohort data where randomization is absent.